
Authors



Hypertrophic cardiomyopathy is the most common inherited cardiac condition and is associated with an increased risk of sudden death in the young. It is frequently associated with symptomatic left ventricular outflow tract obstruction.
Guy’s and St Thomas’ Specialist Care is one of the very few leading centres worldwide with state-of-the-art imaging services, genetic advances and a full range of expert interventions to manage this condition.
Inherited heart muscle conditions (cardiomyopathies)
Globally, the frequency of all inherited cardiac conditions combined is approximately 1 in 100. Tragically, these diseases can potentially lead to sudden death at a young age.
Cardiomyopathy refers to a group of inherited diseases impacting the heart muscle and is prevalent in 1 in 200 in the general population. It can affect people of all ages and is a major cause of morbidity and mortality in younger ages, where other cardiac conditions are uncommon. Being inherited, namely genetic, cardiomyopathies can run in families, affecting several members of a family.
There are major challenges in the diagnosis, treatment and risk prevention in cardiomyopathies and the clinical expertise is concentrated in specialist centres. RB&HH is one of the very few leading centres worldwide offering the full range of expert diagnostics and interventions to manage cardiomyopathies and to lower the risk of sudden death.
Hypertrophic cardiomyopathy (HCM)
HCM is the most common inherited cardiac condition and is characterised by thickening of the heart muscle. Its prevalence is 1 in 500 in the general population and can be associated with sudden cardiac arrest.
On average, 75 per cent of HCM patients have an obstruction in the outflow tract of the left ventricle. Left ventricular outflow tract obstruction (LVOTO) is caused by the thickened heart muscle and the abnormal movement of the mitral valve; this is the main mechanism of symptoms in HCM patients. It is also one of the risk factors for sudden cardiac death, especially in young patients.
Individuals of any age with obstruction in the LVOTO often experience exertional symptoms which can impact daily living and can significantly limit physical activities.
Common signs and symptoms
HCM with LVOTO can manifest itself with any of the following symptoms:
- fatigue
- breathlessness with activity or after lying down (or being asleep for a while)
- lightheadedness, especially with or after activity or exercise
- chest tightness or pain
- fainting or near-fainting, especially during or soon after exercise
- the sensation of feeling the heart beat fast or irregularly (palpitations)
Hypertrophic cardiomyopathy treatment and management services
Management of LVOTO in HCM
When patients get expert treatment, it can result in a substantial improvement in their quality of life.
However, medications used to manage LVOTO have variable efficacy and are sometimes limited by side effects, intolerance or contraindications.
Interventional techniques
Intervention is considered appropriate in patients with a significant degree of outflow obstruction, who are not improving on medication and have symptoms limiting their daily activities.
The two techniques currently available are alcohol septal ablation and surgical myectomy. Before a patient undergoes intervention, they will have a series of tests, including a dynamic echocardiogram and a cardiac MRI, to assess the LVOTO and the anatomy and geometry of both the left ventricle and the mitral valve.
Alcohol septal ablation
Alcohol septal ablation (ASA) is a nonsurgical reduction of the thickness of the ventricular muscle in the area of the outflow tract and is a clinically effective therapeutic option in selected cases.
The procedure involves the tip of a catheter being wedged into a small artery that supplies blood to the thick muscle. Then the area of blood supply is carefully checked with specialised imaging. If appropriate, an infarction is generated in the area by injecting a small amount of ethanol through the catheter. This results in scarring and shrinking of the wall thickness reducing or even eliminating the obstruction. Nevertheless, the improvement may not manifest itself immediately after the procedure.
ASA can only address the muscle thickness and not the other components of the internal anatomy of the heart, and the amount of muscle mass reduction is also limited.
In cases where a large reduction of the wall thickness would be required, it would mean inducing a large myocardial infarction that may increase the risk of the procedure. In general, the risk of major complications is about similar to the risks of major complications with surgery (one per cent). But with ASA, patients benefit from a shorter hospital stay and more rapid recovery.
Surgical myectomy
Septal myectomy entails performing surgical muscle resection (myectomy) to eliminate LVOTO. It is conventionally performed through an incision made through the length of the sternum. This is a complex surgery and is planned carefully with the assistance of specialist imaging, including a transoesophageal echocardiogram (TOE) and cardiac MRI.
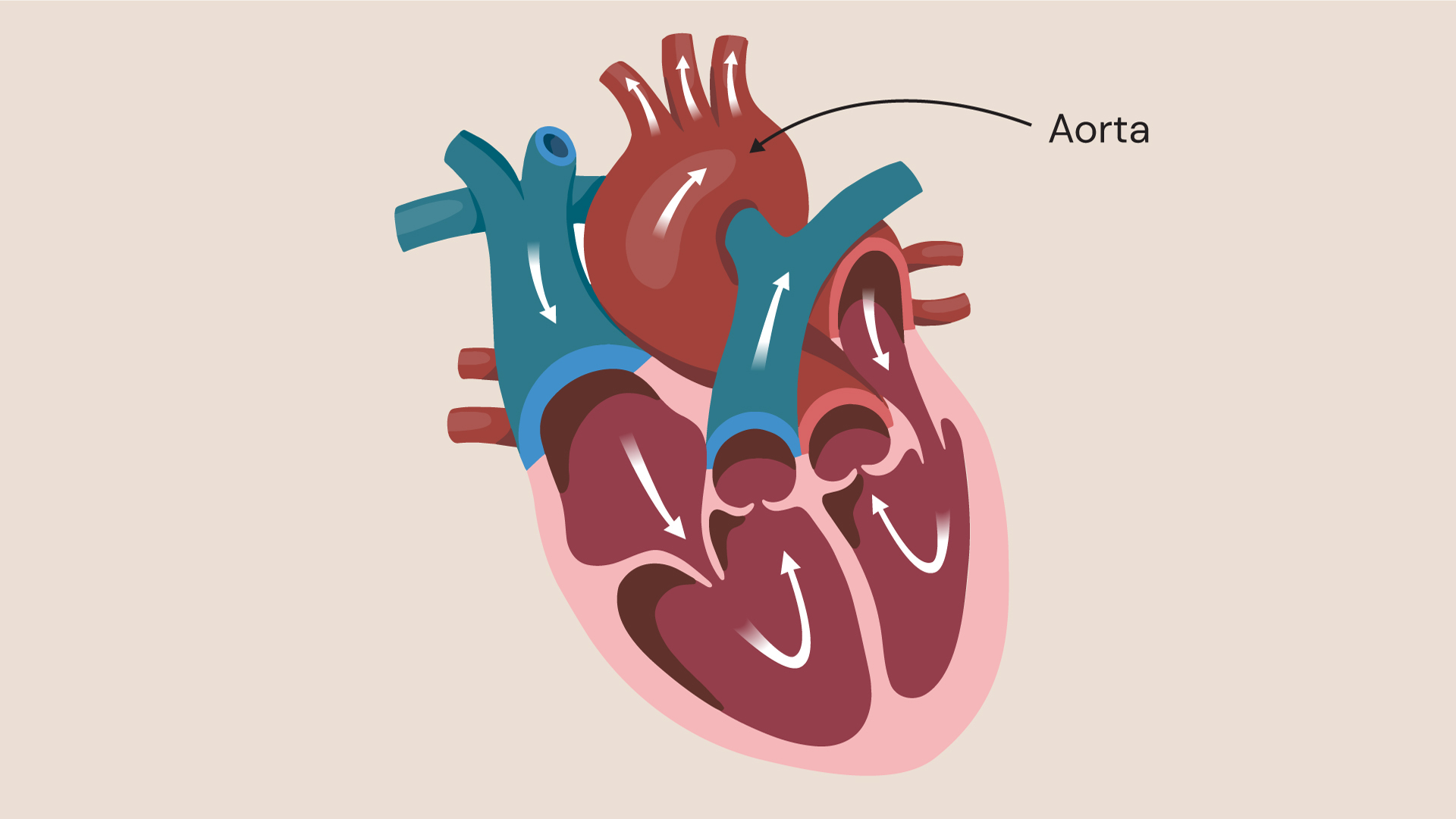
During the procedure, the surgeon will reach the inside of the heart through the aorta and the aortic valve. The inner surface of the heart muscle will then be resected under direct vision in order to relieve the blockage in the areas where it is thickened. The amount of muscle removed varies between 3 and 15g.
The resection is carefully planned and carried out taking into account all the individual anatomical characteristics of the patient’s heart. Even when anatomically normal, the mitral valve contributes to the obstruction and it may hence lose its normal function resulting in leaking blood from the ventricle back to the left atrium.
Mitral regurgitation leads to enlargement of the left atrium and may also lead to atrial fibrillation (AF). Most commonly, the mitral regurgitation is dynamic and releasing the obstruction in the LVOT will also decrease the amount of regurgitation.
Occasionally, the resection of the muscle is not sufficient and then a repair or replacement of the mitral valve may become necessary. This is more likely to be the case when the mitral valve is intrinsically abnormal, a frequent co-factor in Hypertrophic Obstructive Cardiomyopathy (HOCM).
AF is not uncommon in HOCM patients, and if indicated, a surgical AF ablation will be performed at the same time as the myectomy. Following uncomplicated surgery, a patient can be discharged from the hospital within seven days. The relief from obstructive symptoms is rapid but the recovery from the operation may take a while.
Benefits of successful LVOTO management
It is known that LVOTO is one of the risk factors for sudden cardiac death. Although HCM is a condition for which there is not a definitive cure, patients experience major symptomatic improvement after successful management of LVOTO. Data suggest that significant reduction or elimination of LVOTO improves survival and long-term outcome. Longitudinal studies show sustained clinical improvement with 85 to 90 per cent of patients remaining asymptomatic (or only mildly symptomatic), at an average of eight years (and up to 25 years) after a myectomy.
Get in touch
For more information or to book an appointment, please contact our customer care team.
Related content
-
Aortic disease
Aortic stenosis is a narrowing of the aortic valve opening, restricting blood flow to the aorta.
-
Left ventricular outflow tract obstruction (LVOTO)
Left ventricular outflow tract obstruction (LVOTO) is a recognised feature of hypertrophic cardiomyopathy.
-
Valvular heart disease
Heart valve disease occurs when the valves of the heart become diseased or damaged.